 |
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
March 20, 2003 |
URETERO-PELVIC JUNCTION (UPJ) OBSTRUCTION
VALUE OF MR ANGIOGRAPHY IN DIAGNOSING AN ABERRANT CROSSING VESSEL
 |
 |
 |
| Fig.1 | Fig.2 | Fig.3 |
|
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
March 20, 2003 |
|
|
|
| Fig.1 | Fig.2 | Fig.3 |
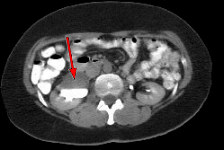
CLINICAL INFORMATION: The patient is a 43-year-old female who presented to the office of a local internist with right flank pain and possible right renal obstruction on prior scans. The patient was referred to AIC for an ultrasound and later CT scan of the abdomen and eventually an MRA of the renal arteries.
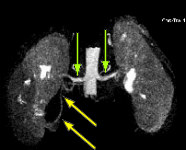
FINDINGS: The ultrasound (not shown) demonstrated dilated collecting system versus extrarenal pelvis on the right. Fig. 1 and Fig. 2 are nephrographic and delayed images through the kidneys. They demonstrate a large dilated right renal pelvis (red arrows) with urine-contrast level and a normal-sized ureter consistent with UPJ obstruction. Fig. 3 is a 3D image from a renal MRA showing an accessory right renal artery (yellow arrows) supplying the right lower pole and impressing upon the right UPJ, explaining the UPJ obstruction. Normal renal arteries are also clearly seen (green arrows)
CAUSES OF UPJ OBSTRUCTION: There are intrinsic and extrinsic causes. Intrinsic causes primarily are due to functional impairment such as due to UPJ muscle anomaly, ischemia or ureteritis. Extrinsic causes include aberrant vessels to the lower pole (such as in the above case), adventitial bands, renal mass or cyst, calculus or aortic aneurysm.
DISCUSSION: There may be other associated anomalies such as VU reflux, ureteral duplication. Neonates presenting with hydronephrosis should be fully evaluated with both a voiding cystourethrogram (VCUG) to rule out vesicoureteral reflux and a renal ultrasound soon after birth. These patients also should also be placed on prophylactic antibiotics to prevent urinary tract infections (UTIs). If renal sonography demonstrates hydronephrosis without reflux on VCUG, a diuretic renal scan (MAG-3, DTPA, or DMSA) should be performed to quantify relative renal function and to define the extent of obstruction. Older children may present with UTIs, a flank mass, or intermittent flank pain secondary to a primary UPJ obstruction. Hematuria also may be a presenting sign if associated with infection. Adults can present with a variety of symptoms, including back and flank pain, UTI, and/or pyelonephritis.
TREATMENT: In children, medical therapy is focused on maintaining sterile urine and assessing renal function and the degree of hydronephrosis for an incomplete obstruction. In both children and adults, surgical intervention (endopyelotomy) to treat a complete UPJ obstruction may be warranted, especially with deterioration of renal function.
For more information, you may call me at (661) 949-8111.
Ray H. Hashemi, M.D., Ph.D.
Director