 |
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
February 14, 2003 |
CT APPEARANCE OF ACUTE PYELONEPHRITIS
 |
 |
 |
| Fig.1 | Fig.2 | Fig.3 |
|
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
February 14, 2003 |
|
|
|
| Fig.1 | Fig.2 | Fig.3 |
CLINICAL PRESENTATION: This 25-year-old female presented to the office of her primary care physician with symptoms of acute right pelvic, right loin, and right lower quadrant (RLQ) pain. Initially, an ovarian pathology was suspected. The patient was referred for imaging studies to AIC. An ultrasound of the abdomen and pelvis (not shown) revealed no IUP or ectopic pregnancy, no free fluid in the pelvis and small ovarian cysts, some possibly hemorrhagic. The kidneys appeared grossly unremarkable without hydronephrosis. The possibility of acute appendicitis was then entertained and a helical CT of the abdomen/pelvis was in order.
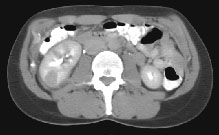
HELICAL CT FINDINGS: The CT was performed on AIC’s multi-slice helical CT (MSCT) scanner. Images with 5 mm collimation were obtained before, immediately following and 5-10 minutes after power injection of IV contrast. The region of the appendix was unremarkable. However, the right kidney and perinephric region were abnormal. Fig. 1 and Fig. 2 illustrate patchy and wedge-shaped low attenuation areas in the right kidney, and Fig. 3 shows stranding/infiltration of perinephric fat around the lower pole consistent with inflammatory changes (arrows).
DIAGNOSIS: The CT images are most compatible with acute pyelonephritis (APN) even without any laboratory results. Shortly after, results of blood work and urinalysis revealed leukocytosis and pyuria substantiating the CT diagnosis.
DISCUSSION: Acute pyelonephritis (APN) is also known as pyelonephritis, acute bacterial nephritis, or acute lobar nephronia and may be diffuse of focal. In adulthood, it is much more common in females than in males. It is caused by infected urine from lower tract with ascending bacterial infection (usually due to a Gram negative organism such as E. Coli > Proteus > Klebsiela, Enterobacter, Pseudomonas, etc.), resulting in upper urinary tract infection with renal pelvic, caliceal and parenchymal as well as perinephric inflammation. Signs and symptoms include fever, chills, flank pain, leukocytosis, microscopic hematuria, and pyuria. IVP is normal in 75% of cases. On CT, the kidneys may be enlarged and postcontrast images may contain areas of lower density due to inflammation and edema, such as in the above case. These areas may slowly fill with contrast resulting in hyperdensity on delayed images up to 24 hours. Loss of corticomedullary differentiation and obliteration of renal sinus fat and caliceal distortion are other CT or ultrasound findings. CT is an excellent modality for diagnosis of APN (even in the absence of lab results) and differentiating it from other causes of right abdominal pain including, but not limited to, urinary stones, appendicitis and acute ovarian/pelvic pathology.
TREATMENT: Prompt antibiotic treatment resolves the infection and leaves no scar in the kidneys.
For more information, you may call me at (661) 949-8111.
Ray H. Hashemi, M.D., Ph.D.
Director