 |
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
October 14, 2002 |
INTERESTING CASE PRESENTATION: Acoustic Neuroma
|
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
October 14, 2002 |
Clinical Presentation: Patient is a 45-year-old female who presented with left hearing loss and dizziness. She was referred to AIC for an MRI of the brain and temporal bones/internal auditory canals (IAC’s … not to be confused with AIC!) with and without gadolinium contrast.
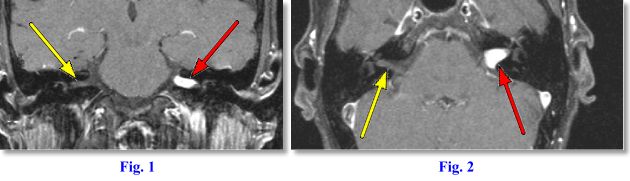
MRI Findings: Figs. 1 and Fig. 2 are thin (2 mm) post-contrast T1 weighted Fat Saturated (fat turns dark) images through the IAC’s performed on AIC’s ultrafast, high-resolution, high-field Siemens Symphony magnet. Fig. 1 is a coronal and Fig. 2 an axial image. They demonstrate a bright enhancing mass in the left cerebellopontine angle (CPA) extending into the left IAC (red arrows). A normal right IAC can be seen (white arrows).
Final Diagnosis: The MR findings are typical of an intracanalicular acoustic neuroma (AN). AN is also called vestibular schwannoma. A meningioma would also be in the differential diagnosis but much less likely, as they tend not to extend into the IAC. Other masses that can occur in the CPA (none of which with this appearance) include arachnoid cyst, metastasis, chordoma, aneurysm, other cranial nerve schawanomas, glomus jugulare, etc. ANs account for 5-7% of all intracranial tumors; 85% of all intracranial neuromas; 80% of all CPA tumors. Most AN’s are purely intracanalicular (95%) with remaining 5% arising at CPA with intracanalicular extension.
Treatment: AN’s may be followed up to rule out enlargement. Average doubling time is about 2 years. Enlarging tumors are surgically removed.
Clinical Symptoms: Unilateral sensorineural hearing loss (AN’s account for 10%), dizziness/giddiness, vertigo, ataxia, unsteadiness, tinnitus, and pain. If tinnitus is also present, a glomus tumor should also be considered. Pulsatile tinnitus is also associated with other vascular lesions such as an aberrant internal carotid artery, dehiscence of jugular fossa, or glomus tympanicum. These latter conditions in and about the middle ear may best be demonstrated on high-resolution axial and coronal CT scan. MRI can also show abnormal fluid in the mastoids or middle ear (serous otitis media). In an older patient, the latter finding should direct the radiologist to evaluate the nasopharynx for possible cancer obstructing the eustachian tube. AN is associated with central neurofibromatosis or NF-2 (95%), contralateral AN (25%) and peripheral neurofibromatosis or NF-1 (5%).
If you have a patient presenting with sensorineural hearing loss, vertigo, tinnitus, and/or dizziness, please consider MRI of the brain plus MRI of the IAC’s (internal auditory canals) / temporal bones with and without contrast. Small AN’s may be missed if contrast is not used or if thin-section cuts through the IAC’s are not obtained.
For more information, you may call me personally at (661) 949-8111. If you have an interesting case, please contact me for a clinical-radiological case presentation.
Ray Hashemi, MD, PhD,
Director