 |
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
July 23, 2001 |
INTERESTING CASE PRESENTATION
Trigger Thumb: MRI Findings
|
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
July 23, 2001 |
CLINICAL INFORMATION: The patient is a 59-year-old female who presented to Dr. Hassan Bacchus* with pain and swelling in the right thumb. She stated, “My thumb jumps in and out of joint.” Clinical diagnosis of trigger thumb was entertained. The patient was referred to AIC for a high-resolution MRI of the thumb to evaluate the status of the flexor tendons.
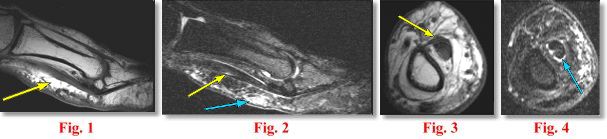
MRI FINDINGS: The MRI was performed on AIC’s high-field 1.5 Tesla short-bore Siemens Symphony. An ultra small, high-resolution digit coil was utilized to evaluate the thumb. A small field of view of only 6 cm was used. Slice thickness of 0.8 mm to 2 mm were selected. Sagittal, axial and coronal 2 mm T1W and fat suppressed T2W Fat Sat and coronal 0.8 mm DESS were obtained. Fig. 1 (Sagittal T1W) shows moderate thickening of the flexor pollicis tendons along the proximal phalanx with some increased signal. Fig. 2 (sagittal T2 Fat Sat) shows the same with subcutaneous edema and small amount of fluid in the tendon sheath. It is difficult to separate the superficial and deep flexor tendons. Fig. 3 and Fig. 4 are the corresponding axial images demonstrating the same findings.
DIAGNOSIS: These findings are c/w tendinitis/tenosynovitis of the flexor tendons typical of a “trigger thumb.”
DISCUSSION: Trigger thumb (or trigger finger) is a condition where the thumb is locked in the flexed position at the interphalangeal (IP) or MCP joint. Sometimes, the thumb can be forcibly extended with a palpable or audible click. Sometimes, it is locked in acute flexion and cannot be extended. Trigger thumb is due to thickening and constriction of the fibrous flexor sheath that surrounds the flexor pollicis tendon pulley at the base of the thumb (stenosing tenosynovitis). Often palpation or pressure of the flexor tendon over the joint can be painful, as can the triggering be painful, and the triggering may get so severe that the thumb or finger gets locked in either flexion or extension and must be, forcefully, brought back to the flexed or extended position using the other hand.
ETIOLOGY: This problem can be the result of repetitive pinching or gripping of the fingers or thumb, as in a repetitive trauma disorder form one’s work and/or hobbies, or may even be the result of direct trauma. It can even occur congenitally, but it is most commonly present in people who either are developing a mild form of arthritis, already have rheumatoid arthritis or another kind of arthritis, or have overused the tendon, so that the covering of the tendon has swollen and gets caught in the pulley system. If the triggering is congenital in origin and does not spontaneously disappear after the first couple of months, it will usually need to be released surgically.
TREATMENT: Initial treatment is conservative such as with the use of non-steroidal anti-inflammatory medications. If these conservative methods are unsuccessful, the trigger finger or thumb will occasionally respond to the injection of a local anesthetic and corticosteroid into the flexor sheath. If surgery is indicated, it can usually be done on an outpatient basis and simply consists of sectioning or dividing the pulley that is entrapping the tendon.
For more information, please call Dr. Bacchus or myself at the numbers below.
Ray H. Hashemi, M.D., Ph.D.,
Director* Dr. Hassan Bacchus, MD, is an internist in Lancaster, California, and can be reached at (661) 948-5086.